Shone’ Syndrome
- A rare congenital heart disease described by Shone in 1963
- Manifests as decreased left ventricular output
- There are two types of Shone’s syndrome: complete and incomplete Shone’s syndrome.
- In the complete form of Shone’s syndrome, all four of the lesions will be present.
In the incomplete form, two or three lesions will be present (more common)
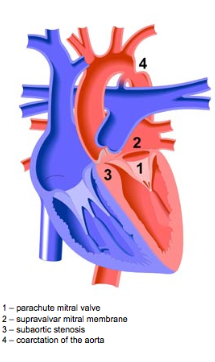
Supravalvular mitral membrane (SVMM): Typically the first abnormality to develop. An abnormal ridge of connective tissue on the atrial side of the mitral valve. Often the supravalvular ring may encroach on the orifice of the mitral valve leaflets and restricts their movements. While a supravalvular mitral ring may allow normal haemodynamic flow from the left atrium to the left ventricle, it often causes an obstruction of the mitral valve inflow(cite). Mitral supravalvular ring is associated with other defects in almost 90% of cases
Valvular Mitral Valve stenosis due to a parachute mitral valve: The mitral valve chordae insert into one papillary muscle. In parachute-like asymmetric mitral valve, most or all chordal attachments are to one papillary muscl. This abnormal attachment of the chordae tendonae results in stenosis of the mitral valve since the valves are held in close proximity.
Subaortic stenosis (membranous or muscular): is a fixed form of anatomic obstruction to outlet of blood across the left ventricular outflow tract. There are four basic anatomic variants which are as follows: (1) a thin discrete membrane consisting of endocardial fold and fibrous tissue, (2) a fibromuscular ridge consisting of a thickened membrane with a muscular base at the crest of the interventricular septum, (3) a diffuse, fibromuscular, tunnel-like narrowing of the LVOT, and (4) accessory or anomalous mitral valve tissue.
Aortic Coarctation: Coarctation of the aorta is a narrowing of the aorta most commonly found just distal to the origin of the left subclavian artery. Since the narrowing occurs distal to the L subclavian artery symptoms typically are manifested in the lower extremities such as cramps, cold feet and decreased ability to perform exercise. Aortic coarctation occurs in 20–59% of cases with mitral valve anomalies
Here is an illustration of the pathology:
Associated Pathologies
Heart failure, pulmonary hypertension, pulmonary edema, right ventricular hypertrophy, Left ventricular hypoplasia, pneumonia and cor pulmonale.
Diagnostic Imaging:
Echocardiogram, Pulmonary Artery catherization, MRI, chest radiograph, heart auscultation, EKG
Clinical Exam/Findings:
Loud S2, cold feet, bilateral rales/crackles. Orthopnea, diastolic murmur, atrial fibrillation, low cardiac output,
Prognosis:
If detected early surgery can be performed to correct the defects and is typically done in stages, which reduce dysfunctions. The longer the patient goes untreated and the more elevated pulmonary artery pressure increases the more worse the outcome.

A happy patient post surgery 🙂
Differential Diagnosis:
Tetraology of Fallot, Cor triastrium sinister, patent ductus arteriousum, bicuspid aortic valve
Works Cited
- Iwata Y, Imai Y, Shin’oka T, Kurosawa H. Subaortic stenosis associated with systolic anterior motion. Heart Vessels. Nov 2008;23(6):436-9.
- Morris et al, CT and MR Imaging of the Mitral Valve: Radiologic-Pathologic Correlation, RadioGraphics, October 2010; 30, 1603-1620.
- Otto CM, Bonow RO. Valvular heart disease. In: Libby P, Bonow RO, Mann DL, Zipes DP, editors. , eds. Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine 8th ed.Philadelphia, PA: WB Saunders; 2007:1625-1712
- Bonow RO, Carabello BA, Chatterjee K, et al. 2008 Focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines Circulation 2008;118:e523-e661.
- Serra W*, Testa P and Ardissino P Mitral supravalvular ring: a case report, Cardiovascular Ultrasound 2005, 3:19
- Popescu BA, Jurcut R, Serban M, Parascan L, Ginghina C. Shone’s syndrome diagnosed with echocardiography and confirmed at pathology, Eur J Echocardiogr. 2008 Nov;9(6):865-7
- Board, A.D.A.M. Editorial. Coarctation of the Aorta. U.S. National Library of Medicine, 18 Jan. 0001. Web. 08 Mar. 2013.
- Brauner R A, Laks H, Drinkwater DC Jr, Scholl F, McCaffery S. Multiple left heart obstructions (Shone’s anomaly) with mitral valve involvement: long-term surgical outcome. Ann Thorac Surg 1997;64:721-9