BUT. It will always be better to be healthy and at a normal weight than healthy and obese. Full stop.
However, we need to stop perpetuating this belief that a lack of motivation is a primary cause of obesity. It’s not. Motivation is a factor to some degree but it’s much less than many of the other societal, environmental and psychological factors relating to obesity.
Too often are obese individuals with various complaints also told to just lose weight. Back pain? Lose weight. Knee pain? Lose weight. Breathlessness? Lose weight.
Cool.
But what are you gonna do for them right now or in the meantime until they lose weight? People need tenable and actionable solutions. They don’t need someone just repeating the obvious or fixating on something that’s a long term goal for what is a much shorter-term problem. Again what are you going to do to help them now?
It takes time to lose weight, especially significant and meaningful amounts. Even 20lbs of body weight is a lot to lose and that’s probably not gonna happen in 1 month (without surgery), and quite honestly probably shouldn’t happen. Weight loss should be sustainable and with realistic goals. For those reasons, successful weight loss is often gradual. Quite often one of the reasons why people fail to lose weight is that they set unrealistic goals for weight loss and get quickly discouraged when they invariably fail to meet to said goals.
In summary, I agree that it’s important to be honest with our patients but let’s perpetuate honesty to our patients.
Oil painting depicting Claude Bernard, the father of modern physiology. (Image Courtesy of Iconographic Collections Keywords: Léon-Augustin Lhermitte; Vivisection; Physiology)
To my student followers struggling with fundamental science coursework: Remember that you are entering a healthcare profession and potentially earning a doctoral degree. A thorough understanding of the fundamental sciences, especially physiology, is necessary for anyone awarded a doctoral degree in the health sciences. This is true for the doctor of medicine degree and it is true for the doctor of physical therapy degree. The performance of our various biological systems dictates physical function and movement. Additionally, a thorough understanding of these systems will allow you to understand the basis for the symptoms and functional limitations present in many of the patient populations physical therapists work within the clinic. Lastly, understanding physiological systems allow physical therapists to prescribe exercise and other interventions appropriately for a patient. So while some of the information learned may seem irrelevant and overly detailed, there is a good reason for it. You may be surprised how many things we do as therapists traces back to a thorough understanding of physiology and other fundamental sciences.
Physiology specifically is also probably the area where most physical therapy students and practicing physical therapists struggle. (I’ve taught both for a few years now.) It’s harder to study/practice and appreciate physiology because you can’t actually “see” many of the things you’re studying, unlike in other areas of the curriculum. But when you start practicing and treating patients with conditions, you’re going to really appreciate the amount of time you spent studying physiology. This is especially true if you work in settings outside of outpatient orthopedics, although physiological principles are very relevant there as well.
As an aside, I’ll also add that a thorough knowledge of physiology will also help with discerning whether and which, continuing education and post-professional training are worth pursuing. There are many approaches to care within our profession which make claims that violate basic concepts of physiology and other accepted sciences. These courses and narratives have perpetuated and promulgated likely in large part due to a lack of understanding (or forgetting) of central tenets from human physiology.
Long story short remembering physiology helps improve your bogus detector. This is important both for you as a clinician and for your patient, who will also be exposed to many of these bogus narratives. So embrace this challenge, like all others in life. You’re going to do fine. No student is ever accepted into any clinical program if the faculty didn’t think they would be successful. And you’re going to be better for having gone through it, like all others challenges in life!
This view might not be too popular among some but it is something that I think is worth mentioning.
I wish more people in our profession dedicated their efforts to creating content that targets the public or is public facing. As someone who oversees some of the largest groups for physical therapists (PTs) (here, here and here) it never ceases to disappointment me by how often PTs create new accounts which basically just repackage previously created content or ideas and then share them to other PTs.
While it is important that we discuss and share information among ourselves as PTs, how many accounts do we need that share the same information and content with dissemination strategies that are really limited just to PT groups? Come on man, at least be original or at least share content beyond the confines of the same PT groups! The real battle is educating and motivating the public (and other professions) to address the many problems facing our healthcare system upstream. It is not creating another for-profit or self-serving PT mentoring group etc.
This is not to lambaste people for creating such groups, accounts or content. Instead it is a call to action to use your creative efforts to take on a larger and more pressing challenge. It also might be to your benefit, the most successful pages and personalities in our profession are those that are more public facing (KStarr, Prehab Guys and Rehab Science just to name a few). From a business and marketing standpoint (in most instances) it is better if your content reaches or is more relatable to a broader audience. Think about it, there are only about ~250K PTs in the USA, while there are 325 million people in the USA (and 3.9 billion internet users worldwide). There is a rather smaller carrying capacity for marketing or sharing content just to other PTs.
To quote the Physiological Society who in 2017 made a similar call to action to scientists:
“In an era of ‘alternative facts’, it is our responsibility that the true (scientifically-evidenced) message is made public rather than allowing rampant myths to be propagated and not challenged by those with access to the wider public, who are, in the end, our target audience. We are in a privileged position whereby a lot of our research can and does have direct application pipelines and as such should reach the end-user directly from us.”
In summary, not only is this more public facing or direct to consumer approach beneficial for improving the status of our profession and potentially your own finances, it will help our patients by offering a discerning voice to the overwhelming amount of nonsense that exists. A light in a world of darkness. A compass in a chaotic healthcare system!
HB 4643 has passed out of committee and will go to the House! This is the closest IL has every been to Direct Access for Physical Therapy Services. Please call the IL reps, even if you aren’t in Illinois. The more states that have direct access, the larger chance the states that do not will move toward it.
The Illinois Chiropractic Society has stated they are against PTs having direct access, mainly since this would put us on a fair playing field. We can pretty much guarantee every Chiro in Illinois will be on the phone to their reps, so lets do the same. All the info you should need is below.
We received great news today as our DIRECT ACCESS BILL PASSED OUT OF COMMITTEE. Now our DIRECT ACCESS bill heads to the House floor and we need your help NOW!
Below is a template letter that we would like you to forward to your House Representative in support of House Bill 4643. The full House will be voting on House Bill 4643 on Thursday or Friday.
Sample message:
I am writing to ask you to vote YES on HB 4643 as amended, which would provide direct access to physical therapists for Illinois residents. This is a practice which is already occurring in 44 states, several of which are not restricted in any way.
The amendments, in summary, provide that a physical therapist may provide services to a patient without a referral from a health care professional for 10 visits or 15 business days whichever occurs first. The bill also ensures that the physical therapist notifies the patient’s treating health care professional within 5 days, ensuring that all health care professionals in the continuum of care are informed of the patient’s treatment plan.
In addition, we have reached an agreement with the dentists and the chiropractors that addressed concerns relating to the treatment of temporomandibular joint disorders and length of care.
This important legislation will provide better and faster access to physical therapy for all populations, including Medicare patients, and will help in the fight against opioid abuse in Illinois, as physical therapy is a non-prescription, non- addictive way to reduce pain.
We appreciate all stakeholders work on this bill as well as the work of legislative staff to bring HB 4643 without any objections from any stakeholders. Please email, call and fax your legislator TODAY. You can find your Representative’s name and contact information, by entering your address at: https://www.illinoispolicy.org/maps/illinois-house/
It is important that every legislator hear our message from many constituents.
The legislation gives the public Direct Access to physical therapists in Illinois. You can access HB 4643, House Amendment 001, 002, 003 at www.ilga.gov. Click on “full text” to read amendment. A new definition labeled 1.2. Physical Therapy Services, allows direct access. There are a few protections for the public and they are reasonable.
According to a retrospective case-control analysis by Taunton et al, of the 2,002 running-related injuries seen at a primary care sports injury facility, 42.1% (842/2,002) were knee injuries. Of these knee injuries, 39.3% (331/842) were due to patellofemoral pain syndrome (PFPS), which made PFPS far and away the most common disgnosis found in this large-scale study. Additionally, an older study done in 1984 showed similar results. Devereaux et al found that over a five year period, 137 patients presented with PFPS, which accounted for 25% of all knee injuries seen at this sports injury clinic. These two studies were conducted 17 years apart, giving support to the consistently high prevalence of this disorder, but the real question is, how are we treating these patients?
Based on a biomechanical study completed by Lieb et al in 1968, the vastus medialis obliquus (VMO) has been the mainstay of most physical therapy…
There was a discussion recently in a Facebook group regarding frustrations with difficult patient encounters and advice on how to best manage these cases. Here below, I have provided a brief list of advice imparted onto me by mentors of mine. Hopefully this helps…..
One of the best pieces of advice a professor of mine gave me was “that you cannot control how people act, you can only control how you react”. This simple quote or credo is so incredibly true and is a great approach to life in general. People can be irrational and their actions frustrating, both of which may become magnified surrounding episodes of poor health.
Another thing to consider, which is a message I’ve adapted from an icon of mine Cael Sanderson, is that every challenge that you face is an opportunity for growth and that we should look forward to challenges; they make us better. Difficult patient encounters are opportunities to learn how to manage difficult patient encounters and it will get easier. It’s also always important to consider that the people we serve could choose elsewhere. They don’t have to be in our clinics. Even in public or federal systems, the patient can still choose to not show up. Take it as a privilege that YOU get to SERVE them and even though they may state that they don’t want to be there, they still decided to show up. Also realize, (and I’ve learned this working with many disadvantaged populations) for many people, even getting to the clinic may be more difficult than you may ever realize.
Regarding verbose patients; there are many people who come to our clinics who have never had the opportunity to speak to a healthcare provider about their problems. Some may not have the opportunity to share their frustrations with anyone who cares or has concern for them. This issue of social isolation and loneliness is a real and growing problem in our modern society. Therefore, consider it a privilege that they are comfortable enough to be verbose with you. Just taking time to listen to them can go a long way. In terms of managing verbosity, because there are time constraints to clinical practice, what I have found to be useful is to try to steer their conversation around the goals for the session or intercede with questions that may help redirect it. Always try to acknowledge what the patient has said before talking, this helps convey that you did listen to them (you really should be), which is important for building trust and rapport. This process can be difficult but it gets easier over time as well.
Regarding patients who are difficult to convince or establish buy-in for your plan of care, especially those who may believe in more liberal interpretations of physiology, be persistent and steadfast but always be respectful and considerate. Remember that few people possess the specific knowledge of human physiology to determine a falsehood from truth as it pertains to disease and 88% of US population is insufficiently healthcare literate. Given these factors, and others it is incredibly difficult to change someone’s views once they have internalized information; ie “You can’t sell meat to vegans and you can’t convince a carnivore to eat vegetables”. If their views interfere with your best judgment as a provider, consider referring them elsewhere; it’s probably best for both. We as a profession and field (healthcare) need to do a better job addressing this process of translating knowledge to our communities both at the clinic level and institutional level. But it all starts with a conversation and re-framing expectations with each individual. At the fundamental level, a clinician is an educator and motivator.
These are just some recommendations and tips. I don’t practice as much now but can recall how difficult it can be in the clinic and realize that things are rarely ideal and we all have our limits. However, if you consider some of these basic principles and perspectives, it helps make difficult situations a bit less stressful when they do occur.
“N=1” is a slogan used to publicise a core purpose of the CauseHealth project. N=1 refers to a project which is focussed on understanding causally important variables which may exist at an individual level, but which are not necessarily represented or understood through scientific inquiry at a population level. There is an assumption that causal variables are essentially context-sensitive, and as such although population data may by symptomatic of causal association, they do not constitute causation. The project seeks to develop existing scientific methods to try and better understand individual variations. In this sense, N=1 has nothing at all to do with acquiescing to “what the patient wants”, or any other similar fabricated straw-man characterisations of the notion which might emerge during discussions about this notion.
A little advice regarding the nature of discussions in this forum and elsewhere:
If one posts anything publicly, or really anywhere to a broad audience, one must realize and understand that individuals will offer both support and criticism. It’s part of the process and not everyone will view things the same way, for many reasons i.e. Knowledge base, biases, experiences etc. Few things in life are dichotomous in nature, where there is an absolute truth and false. Public discussion in any setting is NOT for the meek of heart. If one doesn’t possess the gumption to handle criticisms or contrarian views, they should perhaps reconsider participation in public discussion. Furthermore, if what one posts is so easily criticized, perhaps one should consider heeding the criticisms offered or at least reconsider the merits of what one one has posted. I would also wager (no empirical data to support this, this is based on the multitude of professional discussions and arguments I’ve participated in) that most people who decide to criticize (especially peers) do so out of genuine concern and a desire to improve.
Now I do agree that there should be some ground rules to discussion/argumentation for the sake of decency and purposeful argument, ex. criticisms should be purposeful, valid and follow a sound logical framework. One should also consider how incredibly difficult it is to change someone’s views on any topic, much less when those opposing are steadfast in believing their views to be true and when argument is done via textual mediums of communication. Being outright rude makes that task even more challenging. Why work against yourself? However, not everyone agrees with the same ground rules as I or anyone else; which one must also understand. However, one doesn’t have to respond to criticisms offered either, there’s always a choice.
You could heed this advice or not and continue to become overly offended and attempt to silence others who offer views that differ or continue to be unprofessional in discussions with peers. Ultimately it makes no difference to me, I will still continue to go about how I have regarding discussions. Just some advice. We accomplish little with categorical and unconditional agreement, iron sharpens iron. However, nor do we with shouting matches instead of purposeful, respectful yet incisive discussion.
Also, one should consider entering discussion or argument under the condition that what they argue may be wrong. One should be prepared to argue their point vigorously but be willing to concede when what they argue is shown to not likely be true. If one is not willing to make that concession, there is little point to engage in argument. This is actually a cardinal rule of formal argumentation. This cardinal rule is also something to consider, before posting publicly or one will have a hard time due to the nature of public discussion described above. One should also consider realizing their limits to the value of their opinion and degree of expertise, ie, acknowledge what you know, what you don’t know and that there are people who might be more versed on a given topic. Quick tip, if I engage with someone, I haven’t encountered previously, I usually do a quick search on who they are so I know who I’m discussing with and if I might be out of my league. That’s not to say that we should view the thoughts and opinions of experts dogmatically but it should be in the back of one’s mind that perhaps their opposition might know a bit more on a topic than oneself.
Following some of the conversations that came out the #SocialPT talk I gave at CSM 2017 with Ben Fung, Greg Todd and Brett Kestenbaum, (video via UpDoc Media), I felt it would be useful to create a resource to help students and clinicians stay up to date with the evidence. As an emerging researcher and academic, I am passionate about serving this profession as both a purveyor and guide of knowledge to help inform the care provided in our communities. No more ivory towers and no more “knowledge obscura”. We are all our profession’s keeper and the better informed we all are individually, the better off our profession will be collectively. In the list below, I have provided 10 easy tips to help clinicians and students stay current through a variety of different methods, many of which only require a small addition to a typical day. 90% of them are completely free and 100% are of no additional cost for APTA members. Choose one or choose all 10!
PT Now is a resource designed for APTA members which provides summary findings on clinical questions, access to clinical practice guidelines, validated outcome measures and an article search function. Also be sure to check out the APTA PT Outcomes Registry. This project will allow clinicians to participate in the research process by contributing outcomes data to a national registry. The data from this project will be instrumental in advancing care for our patients and creating leverage with legislators and policy makers.
2) Create a PubMed MyNCBI account and create saved searches (free)
This will allows users to track research topics, questions or relationships that interest them. Users can then schedule email reminders on these topics as new papers are published. Though these are only abstracts, it’s a good start and often once the PubMed link is obtained most people have an easier time finding the manuscript. There are also many articles available through PubMed Central, a database designed to host biomedical information free to the public. I have included a YouTube video of how to set up a MyNCBI account and saved searches as well as a step by step instruction with pictures.
YouTube Demo
How to set up “saved searches”
Step 1. Create a MyNCBI account
Step 2. After creating a MyNCBI account, log in and perform a search on a topic that interests you; i.e. “Back Pain”
Step 3. After the search is performed, click on “Create Alert”
Step 4. Create a saved search with scheduled reminders delivered to your email at a frequency of your choosing.
3) Push notifications” from Journal Twitter accounts
This will push notifications to your phone whenever the Twitter account for a selected journal posts. Many of these Twitter accounts also have public “lists” of journals, clinicians and researchers they follow which may help structure your search, as an examples the Cardiopulmonary Section’s Twitter Account has two (one cardiac and one pulmonary/critical care). I have included a step by step instruction with pictures for both.
How to “Push Notifications on Twitter”
Step 1. Click/tap on the notifications icon
Step 2. Select “All Tweets”
How to subscribe to a “list” on a Twitter account
Step 1. Click/tap on the settings button.
Step 2. Select view lists
Step 3. Select a list you would like to subscribe to.
Step 4. Click/tap “subscribe”
4) Subscribe YouTube channels and Podcasts (free)
These platforms provide synthesized content on research or clinical topics. The content on podcasts will generally be audio only and Youtube Channels will usually use both visual and audio. These resources are great since they can be listened to while doing something else, such as the ride to and from work or while exercising. Podcasts are particularly great because if users have the podcast app for iTunes, updates to podcasts they subscribe to are automatically pushed to their phone. I have compiled a good list of YouTube Channels and Podcasts for physical therapists here but be sure to perform your own search to find channels or podcasts that interest you. A few of the YouTube channels I subscribe to are the New England Journal of Medicine, British Journal of Sports Medicine and Heart by the British Medical Journal. Also don’t forget to check out the Cardiopulmonary Physical Therapy Journal Podcast!
5) Register/Subscribe to a journal email list (free)
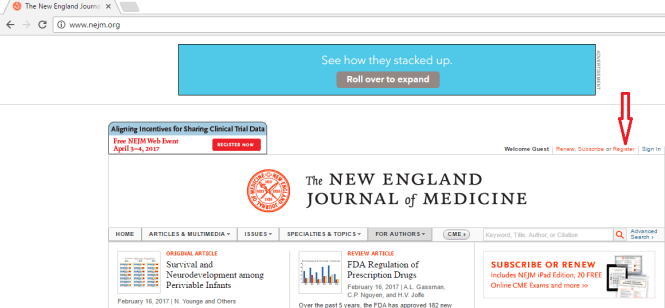
This allows users to receive an updates on new publications and papers published ahead of print. I have provided a step by step example for how to do it through the New England Journal of Medicine, a journal that also often publishes open access (free) manuscripts.
How to “Register/Subscribe to a journal email list”
Step 1. Click “Register”
Step 2. Fill in your email and select a password to register. A confirmation email will be sent to you.
Step 3. Select the “content alerts” and specialty areas you would like to receive emails about. Some journals may not have multiple options.
6) Follow Facebook pages for journals (free)
This tip is similar to “pushing notifications” for twitter. However, an advantage of doing this through Facebook is that more people both have Facebook accounts and check them daily than Twitter. One of the easiest ways to keep up to date with the evidence is make it a component of your daily life.
How to “Push Notifications on For a Facebook Page”
Step 1. Click on the “Following” button
Step 2. Click/Tap the notifications tab, then under “Posts” select receive notifications from “All Posts”
Step 3. Click/Tap the “News Feed” Tab and choose “see notifications from this page on your timeline first”. This places posts from this page at the top of your timeline (not necessary but useful for many)
7) Follow individual researchers (free)
Many researchers have social media accounts and a large portion of them are fairly active, especially on Twitter I actually made a list of some of these accounts worth checking out. Users can also, “push notifications” from their accounts too! I would also recommend signing up for researchgate, this site is increasingly being used by both researchers and clinicians alike. On this site many researchers provide full texts of their papers that can be downloaded, usually 1 year post publication. Users can also request papers from researchers that aren’t publicly available yet on researchgate.
8) Join in the discussions on twitter (free)
To join in these discussions follow hashtags such as #solvePT or #BackPain. To be more specific, I would also recommend using Symplur , a free healthcare hashtag aggregator to help find topics that interest you and even monthly twitter journal clubs such as BMJ Heart’s “Heart Journal Club” #HeartJC .
9) Join in discussions on Facebook groups (free)
One of the best ways to stay informed is to regularly participate in professional discourse. This allows clinicians to appreciate different perspectives from colleagues and to have their biases potentially challenged. Even if you don’t participate, observing some of the discussions from a distance can be useful too! Doctor of Physical Therapy Students or Physical Therapy Practice Education and Networking are two of the largest and most active groups. These groups are also great for asking questions and sharing information.
10) Create a system to manage your citations (free)
As you begin to accumulate resources, especially published work it is important to keep track of them in an organized fashion. This allows you to quickly reference papers and to search for them later. I use Mendeley and Google Drive; both are free to use and excellent software solutions! Mendeley also offers a google chrome extension that allows me to cite resources as I browse. Google Drive has a desktop app that allows me to save files locally on my hard-drive while also continuously and simultaneously pushing files to a cloud based folder which can be accessed anywhere with internet access; even on my phone with the Google Drive App.
I hope these quick tips will provide a better infrastructure for both finding research papers and regularly consuming evidence. If we are all individually more up to date with the scientific literature, better informed decisions can be made for the people and communities we serve!